Introduction
Degenerative foraminal stenosis is an important consideration in endoscopic spine surgery. Progressive anatomical changes within the lumbar foramen can significantly alter the available surgical corridor used during transforaminal procedures.
Successful surgical planning requires a detailed understanding of how degeneration modifies foraminal dimensions, neural relationships, and instrument feasibility.
Why scope size matters: In endoscopic spine surgery, the instruments must fit through the natural opening of the foramen. When the foramen becomes tight from arthritis and disc collapse, smaller endoscopes may allow access with no bone removal, while larger systems require bone removal just to create room for safe insertion.
For background, see Lumbar Foramen Anatomy
Pathophysiology of Degenerative Foraminal Stenosis
Degenerative foraminal stenosis develops through a combination of structural changes:
- Loss of disc height
- Facet joint hypertrophy
- Osteophyte formation
- Ligamentous thickening
- Segmental instability
As disc height decreases, the vertical dimension of the lumbar foramen is reduced. Simultaneously, facet overgrowth narrows the posterolateral corridor, further compromising the safe working zone.
These progressive changes diminish both neural space and surgical access.
Anatomical Consequences Within the Lumbar Foramen
The lumbar foramen is a dynamic structure rather than a static opening. Degeneration produces:
- Reduced vertical clearance
- Decreased horizontal width
- Altered nerve root orientation
- Increased neural compression risk
These changes directly impact the geometry of the transforaminal corridor and may distort the classical boundaries described in Kambin’s triangle.
Therefore, degenerative stenosis affects not only symptoms but also surgical strategy.
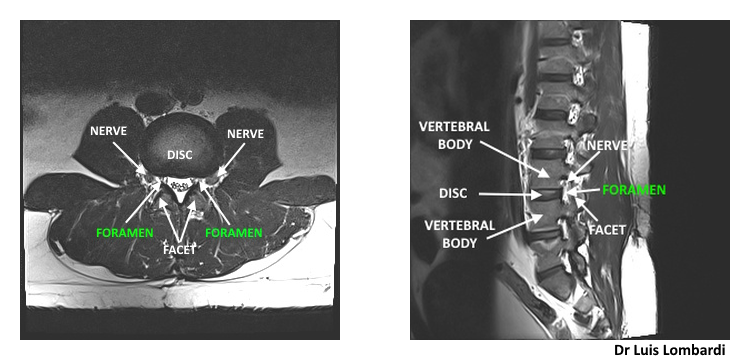
These axial and sagittal MRI views show the lumbar foramen and its normal corridor dimensions, which form the anatomical basis for transforaminal endoscopic access planning.
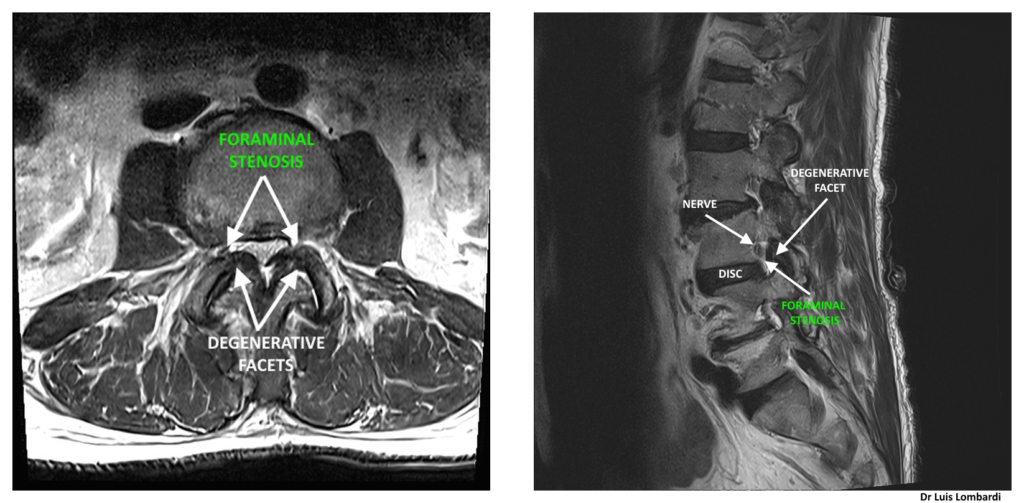
These views illustrate degenerative foraminal stenosis with narrowing of the foraminal corridor, which directly impacts endoscope diameter selection.
Impact on Endoscopic Transforaminal Access
In patients with degenerative foraminal stenosis, the natural surgical corridor may be substantially narrowed. Narrowing directly affects the geometry of Kambin’s triangle.
This influences:
- Endoscope diameter selection
- Cannula positioning
- Surgical trajectory
- Need for facet resection
Instrument size can change the plan. Larger-diameter systems may require access-enabling bone removal to create enough room to insert the endoscope safely. Smaller endoscopic systems pass through restricted corridors without bone removal while still treating the pathology.
The choice must be guided by anatomical constraints rather than procedural preference.
Role of Preoperative Imaging
Preoperative MRI and CT imaging are essential in cases of degenerative foraminal stenosis.
Imaging allows evaluation of:
- Degree of disc collapse
- Facet hypertrophy severity
- Foraminal width
- Osteophyte encroachment
- Neural compression
Imaging also helps the surgeon estimate whether the corridor can accommodate the planned endoscope size.
Individualized planning is particularly critical in advanced degeneration.
Surgical Strategy: Preservation
The surgical objective is to achieve adequate treatment of the pathology while preserving spinal stability.
Decision-making includes:
- Selecting an endoscope size that matches the available corridor
- Using the smallest effective system when anatomy is tight, to reduce the need for bone removal
- Avoiding unnecessary bone removal that could affect stability
Precision planning minimizes risk and optimizes outcomes.
Conclusion
Degenerative foraminal stenosis significantly alters lumbar foraminal anatomy and directly influences surgical planning in endoscopic spine procedures.
Understanding the anatomical consequences of disc collapse and facet hypertrophy is essential for selecting instrument size and planning trajectory.
Frequently Asked Questions About Degenerative Foraminal Stenosis
What causes degenerative foraminal stenosis?
It results from age-related structural changes such as disc height loss, facet arthritis, and osteophyte formation that progressively narrow the lumbar foramen.
Does degenerative stenosis always require facet removal?
Not always. The need for facet resection depends on the degree of narrowing and the required surgical corridor. Careful imaging evaluation determines the appropriate approach. Smaller endoscopes do not require facet removal, even in degenerative foraminal stenosis.
Can a smaller endoscope reduce the need for bone removal?
Yes. When the foramen is narrowed, a smaller endoscope may fit through the available space with no bone trimming.
More on Lumbar Foraminal Anatomy
Understanding the Lumbar Foramen in Endoscopic Spine Surgery
Kambin’s Triangle: Anatomical Boundaries and Surgical Implications in Endoscopic Spine Surgery
Endoscope Diameter and Foraminal Access in Endoscopic Spine Surgery