Introduction: Why Endoscope Diameter Matters
Endoscope diameter is not a minor technical detail in endoscopic spine surgery. It directly affects whether the natural lumbar foraminal corridor is sufficient—or whether bony removal becomes necessary.
In transforaminal endoscopic approaches, safety is determined by the interaction between foraminal anatomy, the working cannula diameter, and the required surgical trajectory. Understanding that relationship helps optimize nerve safety and preserve facet integrity.
See Lumbar Foraminal Anatomy for the full cluster
Endoscope Diameter and the Foraminal Working Corridor
The lumbar foramen offers a limited surgical corridor. The usable working space varies with:
- Disc height
- Facet orientation
- Foraminal dimensions
- Degenerative narrowing
- Endoscope and cannula diameter
As instrument diameter increases, the corridor required for safe passage increases. When native space is insufficient, corridor expansion—often through facet resection—may be required.
By contrast, smaller-diameter endoscopes can work within tighter corridors while preserving native bony anatomy.
Working Cannula Diameter, Scope Size, and 3D Foraminal Constraints
The transforaminal working corridor is a three-dimensional space, not a flat triangle. With increasing cannula diameter:
- Clearance within Kambin’s triangle decreases.
- The risk of proximity to (or compression of) the exiting nerve root increases.
- The superior articular process becomes a dominant limiting boundary in the posterolateral corridor.
- The margin of safety narrows.
Even small differences in cannula size can meaningfully change the trajectory required to maintain safe neural distance. Instrument selection should therefore match patient-specific foraminal anatomy, not habit.
Endoscope Diameter, Facet Removal, and Safe Transforaminal Access
Facet removal is considered when:
- The foraminal corridor cannot safely accommodate the chosen cannula
- Degenerative hypertrophy narrows posterolateral access
- The planned trajectory risks neural contact or compression
- The target pathology cannot be reached without enlarging the corridor
Larger endoscopic systems require facet removal to create adequate clearance. Smaller systems fit even in narrowed corridors without bone removal.
The decision is anatomical—not procedural.
Degenerative Foraminal Stenosis: Choosing Endoscope Diameter and Cannula Size
Degeneration changes both corridor size and feasibility:
- Disc height loss reduces vertical clearance
- Facet arthrosis narrows posterolateral access
- Osteophytes and hypertrophy can constrain trajectory options
In advanced degeneration, selecting a smaller endoscopic system allow safer access while preserving spinal stability and reducing destabilization risk.
Imaging Planning: Matching Endoscope Diameter to Foraminal Anatomy
Preoperative MRI and CT can help evaluate:
- Available foraminal width and height
- Degree and location of facet hypertrophy
- Nerve root–disc relationship
- The most realistic working trajectory
Whenever possible, instrument selection should follow objective anatomical assessment rather than preference. Planning based on measurements can reduce unnecessary bone removal and support tissue preservation.
Preservation Strategy: Smaller Endoscope Diameter vs Larger Systems
The objective in lumbar transforaminal endoscopic surgery is not merely to enter the foramen. The goal is to reach the pathology—disc, foramen, or canal—with maximal preservation of normal structures.
Choosing the right endoscope diameter can:
- Reduce the likelihood of facet removal
- Minimize destabilization risk
- Maintain anatomical integrity
- Support postoperative recovery
Endoscope diameter is therefore a strategic variable in surgical planning, not a footnote.
Conceptual Comparison: Smaller vs Larger Endoscopic Systems (Transforaminal Access)
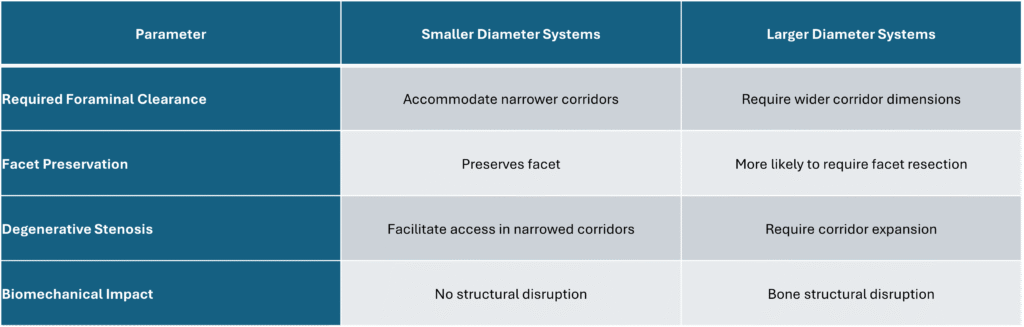
Table 1. Scope Size and Foraminal Access: Operative Considerations
Frequently Asked Questions: Endoscope Diameter and Foraminal Endoscopic Surgery
Does endoscope diameter determine foraminal access?
Larger systems are more likely to require partial facet resection when the natural foraminal corridor is limited.
Can smaller endoscope diameter preserve the foraminal corridor?
Yes. Smaller-diameter systems allow access through narrower corridors while preserving facet anatomy.
How do surgeons decide which endoscope size to use?
Based on imaging, available foraminal dimensions, the planned trajectory, and the degree of degenerative narrowing affecting access.
Internal links
To understand why corridor size varies so much between patients, also see:Lumbar foraminal anatomy
- Lumbar foraminal anatomy
- Degenerative foraminal stenosis: what it means and how surgeons plan endoscopic access
- Kambin’s triangle explained: the safe zone used in transforaminal endoscopic surgery
- Understanding the Lumbar Foramen in Endoscopic Spine Surgery
Conclusion: Endoscope Diameter and Foraminal Endoscopic Surgery
In transforaminal endoscopic spine surgery, endoscope diameter and lumbar foraminal anatomy together determine whether facet removal is necessary. Smaller systems enable preservation of native anatomy, while larger systems require corridor expansion through bone resection.
Best outcomes come from individualized anatomical assessment, deliberate trajectory planning, and selecting instrument diameter to match the patient’s foraminal constraints.