Lumbar foraminal anatomy in endoscopic transforaminal surgery
Lumbar foraminal anatomy is central to endoscopic transforaminal spine surgery. Anatomic variability, degenerative changes, and instrument selection (including endoscope diameter) directly influence surgical access and neural safety. This hub organizes the core concepts that define the working corridor—so each article in the cluster fits into a single planning framework.
What this cluster covers
This series focuses on the anatomy and constraints that shape transforaminal access, including:
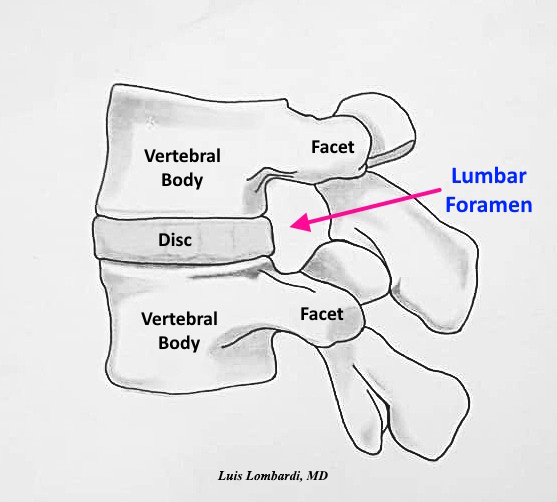
The anatomic boundaries of the lumbar foramen that define clearance and risk
Kambin’s triangle as a corridor concept and how it varies by level and degeneration
Degenerative changes that narrow access (disc height loss, facet hypertrophy, osteophytes)
How endoscope diameter / cannula size influences corridor requirements and the likelihood of facet work
Core Articles in This Cluster
Understanding the Lumbar Foramen in Endoscopic Spine Surgery
Kambin’s Triangle: Anatomical Boundaries and Surgical Implications in Endoscopic Spine Surgery
Degenerative Foraminal Stenosis and Surgical Planning in Endoscopic Spine Surgery
Endoscope Diameter and Foraminal Access in Endoscopic Spine Surgery
FAQ: Lumbar foraminal anatomy
What does “foraminal corridor” mean in transforaminal endoscopy?
It refers to the three-dimensional space used to reach the target pathology through the foramen while maintaining safe distance from the exiting nerve root and avoiding unnecessary facet disruption.
Why does degeneration change access?
Disc height loss and facet hypertrophy reduce clearance and constrain trajectory, sometimes requiring corridor enlargement to maintain neural safety.
How does endoscope diameter influence access?
Larger cannulas require more clearance and increase the need for facet undercutting, while smaller systems preserve bony anatomy in tighter corridors.