Introduction
Kambin’s triangle is a key anatomical landmark in endoscopic spine surgery and represents a critical component of the lumbar foramen used during transforaminal access. It is a corridor to access the disc and the spinal canal. Understanding its boundaries, anatomical variability, and surgical limitations are essential for safe and effective endoscopic spine surgery.
Although traditionally described as a triangular safe zone, its dimensions are not fixed. Patient-specific anatomical variations and degenerative changes significantly influence the true working space available during surgery.
Related reading: Foraminal anatomy
Kambin’s Triangle endoscopic surgery boundaries
Kambin’s triangle is defined by three primary anatomical structures:
- Hypotenuse: Exiting nerve root
- Base: Superior endplate of the caudal vertebra
- Height: Descending nerve root
This triangular corridor provides a pathway to the posterior disc and the spinal canal without direct retraction of neural elements when appropriate technique and trajectory are used.
However, the shape may be more trapezoidal or irregular rather than perfectly triangular, especially in degenerative conditions.
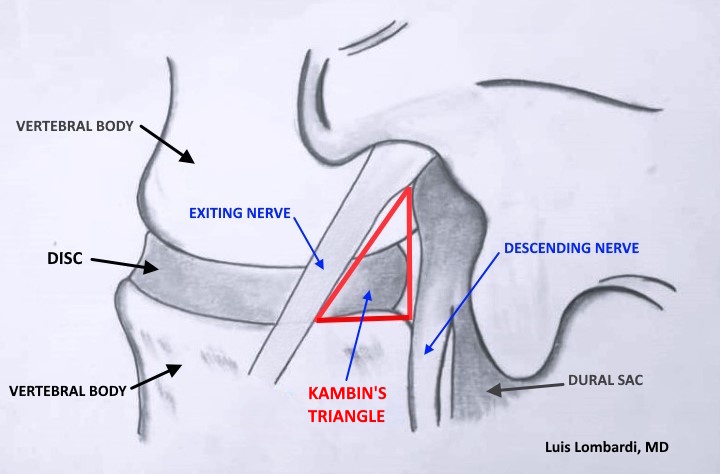
The triangular corridor illustrated above represents the transforaminal access zone within the lumbar foramen used in endoscopic spine procedures.
Instrument feasibility within this space depends on anatomical dimensions and appropriate endoscope diameter selection.
In cases of degenerative foraminal stenosis, the available working corridor may become significantly restricted.
Level-Specific Variability in the Lumbar Spine
The dimensions of Kambin’s triangle vary significantly between lumbar levels:
- Upper lumbar levels tend to have smaller working corridors.
- L4–L5 often provides more favorable access due to relative disc height.
- L5–S1 may be constrained by iliac crest height and facet orientation.
Because of these anatomical differences, measurements reported in morphometric studies should be interpreted as reference values rather than absolute surgical limits.
Impact of Degeneration on the Triangular Safe Zone
Degenerative processes alter the anatomy of the lumbar foramen and directly affect Kambin’s triangle:
- Disc height loss reduces vertical working space.
- Facet hypertrophy narrows the corridor.
- Degenerative Foraminal stenosis decreases safe instrument passage.
- Ligamentous thickening further restricts access.
These degenerative changes directly affect the overall dimensions of the lumbar foramen, further influencing the available working corridor. As degeneration progresses, the triangle may become significantly smaller or distorted, requiring modification of surgical strategy.
Kambin’s Triangle endoscopic surgery corridor
Successful transforaminal endoscopic surgery depends on:
- Accurate preoperative imaging analysis (MRI and CT)
- Proper trajectory planning
- Selection of appropriate endoscope diameter
- Determination of whether facet resection is necessary
Large endoscopic systems may require facet removal to create adequate working space. In contrast, small-diameter endoscopes can often preserve native bone anatomy while maintaining safe access.
A broader understanding of the lumbar foramen and its anatomical variability is essential when planning endoscopic access strategies. Therefore, the concept of a universal “safe zone” must be replaced with a patient-specific anatomical assessment.
Imaging Evaluation and Preoperative Planning
MRI and CT imaging are essential to evaluate:
- Foraminal dimensions
- Relationship of nerve roots
- Degree of facet overgrowth
- Disc height preservation
Preoperative assessment allows the surgeon to anticipate technical challenges and choose the least invasive approach.
Anatomical precision directly correlates with surgical safety and effectiveness.
Frequently Asked Questions About Kambin’s Triangle
What is Kambin’s triangle in spine surgery?
Kambin’s triangle is the anatomical corridor within the lumbar foramen used during transforaminal endoscopic spine surgery to access the disc and the spinal canal.
Does Kambin’s triangle have the same size in all patients?
No. Its dimensions vary by spinal level, patient anatomy, and degree of degeneration. Preoperative imaging is required to determine the safe working space.
When is facet removal necessary?
Facet resection is considered when the natural foraminal corridor is insufficient to safely accommodate surgical instruments, particularly when using larger endoscopic systems.
Conclusion
Kambin’s triangle remains a fundamental anatomical concept in endoscopic transforaminal spine surgery. However, its dimensions are dynamic rather than fixed. Degeneration, anatomical variability, and instrument size all influence the true safe working corridor.
In modern endoscopic transforaminal spine surgery, individualized anatomical assessment—not reliance on textbook measurements—forms the foundation of safe and effective surgical intervention.
More on Lumbar Foramen Anatomy:
If you’d like to go deeper into lumbar foramen anatomy and how it affects endoscopic planning, these articles expand on the key concepts:
Degenerative foraminal stenosis: what it means and how surgeons plan endoscopic access
Endoscope Diameter and Foraminal Access in Endoscopic Spine Surgery
Understanding the Lumbar Foramen in Endoscopic Spine Surgery